| **IN THIS GUIDE** |
|---|
| What vision billing is and how it differs from medical billing |
| Which vision plans matter most for independent OD practices |
| The CPT codes every optometry practice bills |
| How coordination of benefits works and when to apply it |
| The five billing mistakes that cost practices the most revenue |
| How to fix the routing decision at the source |
Vision Billing in Optometry: The Complete 2026 Practice Guide
Last updated: July 17, 2026
Vision billing is the simpler of the two billing systems independent optometry practices run. That is what makes it the most dangerous.
Because it feels manageable, most practices build their entire billing workflow around it. Open the portal, verify eligibility, submit the claim, collect the payment. It becomes muscle memory. And that is exactly when the routing check stops happening.
That works fine. Until a diabetic patient gets routed to VSP at check-in and the practice collects $65 on a visit that qualified for significantly more on medical insurance. No denial arrives. The claim closes. That difference is just gone, with no record it ever happened.
For the complete guide on fixing the routing decision at intake, see the complete optometry billing guide. To see how GIMBL automates this decision before a claim is built, visit gimbl.io.
**What Is Vision Billing in Optometry?**
Vision billing means submitting claims to vision benefit plans for routine eye care services and collecting payment on them.
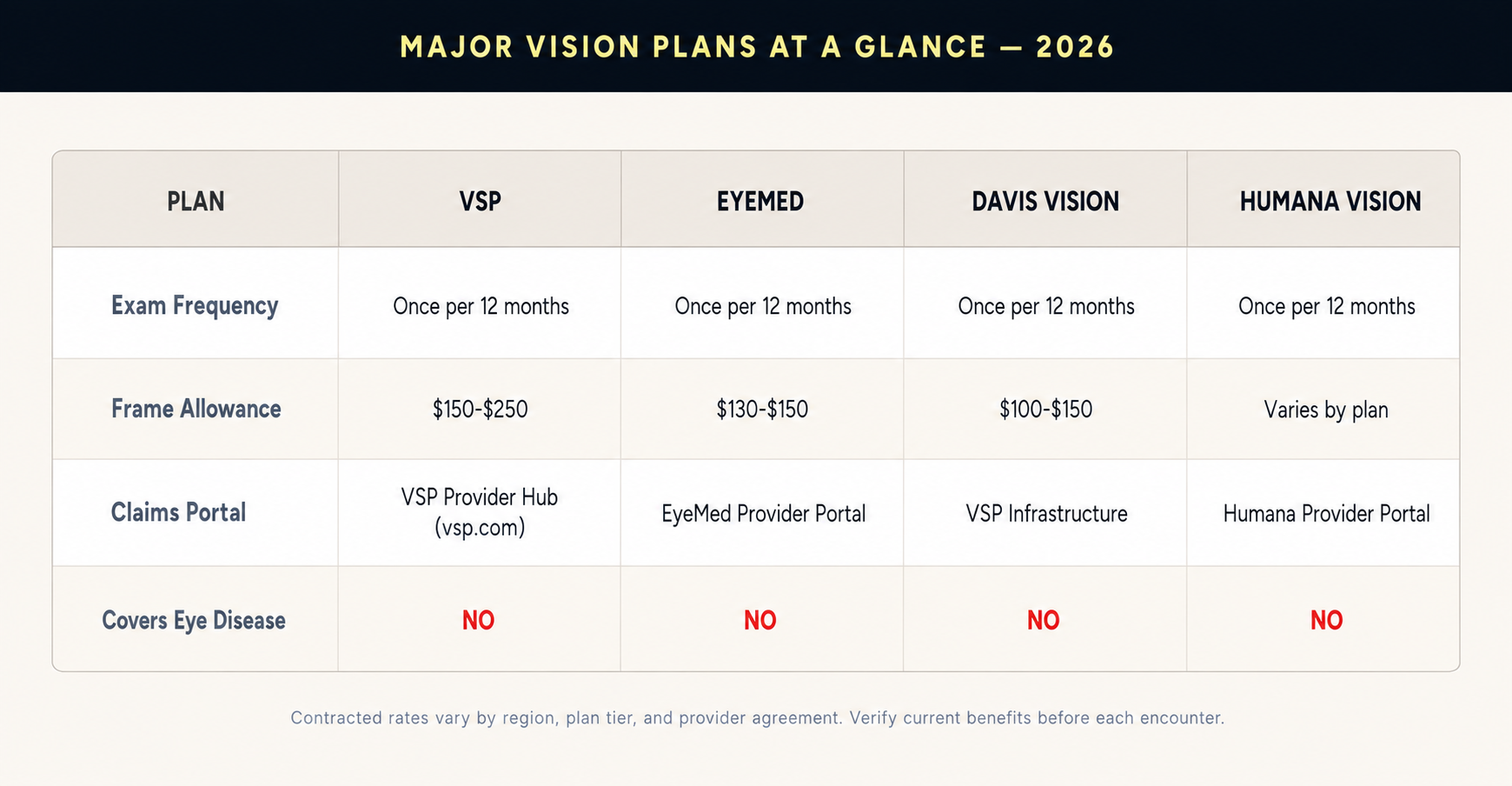
The major plans are VSP, EyeMed, Davis Vision, Superior Vision, and Humana Vision. They cover annual eye exams, refraction, contact lens fittings, frames, and lenses. Reimbursement rates are negotiated by contract and vary by plan, region, and provider tier.
That is the entire scope. Vision billing is for wellness encounters. It is not for disease. It is not for injury. The moment a visit involves a diagnosable eye condition, vision billing is the wrong system and filing to a vision plan will either result in denial or silent underpayment at the wrong rate.
KEY TAKEAWAY: Vision billing is for wellness. Medical billing is for disease. The chief complaint determines which system applies, not the insurance card the patient hands over at check-in.
Vision Billing vs Medical Billing: Key Differences
Most of the expensive billing errors in independent optometry trace back to one decision: choosing the wrong system for a given encounter. This table shows the key differences between the two billing worlds.
The same patient can have both billed on the same day when distinct services are performed and separately documented. A dry eye evaluation goes to medical insurance. A refraction performed in the same visit goes to the vision plan. That is Coordination of Benefits and most independent practices are not doing it systematically.
The billing medical vs vision decision is not a billing function. It happens at check-in before billing starts. Most practices have nothing written behind it, which means it depends on whoever showed up that morning.
KEY TAKEAWAY: The reimbursement gap between the two systems on a qualifying encounter is significant. Practices that consistently route medical encounters to vision plans are leaving revenue on the table on every qualifying visit, with no denial to flag it.
For the complete breakdown including the decision tree and 5-question intake script, see the complete optometry billing guide.
Vision Insurance Plans for Optometrists (VSP, EyeMed, Davis and More)
Every major vision plan has its own portal, its own contracted fee schedule, its own frequency rules, and its own denial patterns. Here is what independent OD practices need to know about each one.
**VSP (Vision Service Plan)**
VSP is the largest vision benefit organization in the United States with more than 80 million members. Most independent OD practices bill VSP through the provider hub at vsp.com. VSP does not operate through the standard CMS-1500 form or clearinghouses.
VSP covers comprehensive eye exams once per 12 months, refraction included in most plans, frames at a plan-specific allowance, lenses in full for standard options, and contact lenses in lieu of glasses. VSP does not cover eye disease treatment, urgent eye care, or any encounter requiring a medical ICD-10 code.
For the full workflow, portal steps, and codes, see the VSP billing guide for optometrists.
**EyeMed Vision Care**
EyeMed covers approximately 75 million members and is owned by Luxottica. The critical difference from VSP is benefit variability. EyeMed plan benefits differ significantly by employer group. Verify specific benefit details before every EyeMed encounter, not just at new patient intake. Claims submit through the EyeMed provider portal.
**Davis Vision, Superior Vision, and Humana Vision**
Davis Vision and Superior Vision were both acquired by VSP Global and are migrating to VSP infrastructure. Confirm which portal applies for your specific credentialing before submitting.
Humana Vision requires specific attention because Humana offers vision coverage both as a standalone product and as part of Medicare Advantage plans. When a Humana Medicare Advantage member presents, determine whether the encounter is routine or medical before selecting which plan receives the claim. A medical encounter goes to the Medicare Advantage plan, not Humana Vision.
KEY TAKEAWAY: VSP and EyeMed together cover the majority of vision plan encounters in most independent OD practices. Every plan has unique portal requirements. Never assume one portal workflow applies to another plan.
Vision Plan Frequency Limits by Insurer (2026)
Every vision plan limits how often a patient can use their benefit. Verify current eligibility before every encounter without exception.

Note: All frequency limits vary by employer group and plan tier. The table shows typical commercial plan limits. Always verify.
The frequency limit trap: when a medical encounter gets routed to the vision plan, the annual exam benefit gets consumed on a visit that should have gone to medical insurance. The patient returns later in the plan year for their actual routine exam and the benefit is exhausted. The routing error from months earlier becomes a patient relations problem today.
Vision Billing CPT Codes for Optometrists
Vision billing uses specific CPT codes exclusive to eye care providers. These are the most important ones and the errors that happen when they are used incorrectly.
92002 — Intermediate exam, new patient. Anterior segment focus, no dilated fundus evaluation.
92004 — Comprehensive exam, new patient. Includes dilated fundus evaluation. Most common new patient code.
92012 — Intermediate exam, established patient. For follow-up and monitoring visits.
92014 — Comprehensive exam, established patient. Most commonly billed established patient code.
CRITICAL: A patient not seen by any provider in your practice within the past 36 months qualifies as a new patient. Billing 92014 for a patient who qualifies as new results in reduced reimbursement or denial. Check new vs established status on every patient at every visit without exception.
92015 — Refraction. Never covered by Medicare under any circumstances. Bill to vision plan or collect directly from the patient. Get an ABN signed before the exam for Medicare-only patients.
92310-92317 — Contact lens fitting codes by lens type. Some plans require prior authorization. Verify at time of scheduling.
V2020-V2599 — Optical dispensing V-codes for frames, lenses, and contacts. VSP uses its own internal code structure through the portal. Do not use standard V-codes outside the VSP portal workflow.
Modifier 25 — Required when a comprehensive eye exam and a procedure are performed on the same day. Without it the payer bundles both and pays for one. The missed revenue never triggers a denial.
Source: AMA CPT Reference | AAPC Optometry Codes
KEY TAKEAWAY: The two most consistently missed CPT rules in vision billing: billing 92014 for patients who qualify as new (36-month rule), and billing 92015 to Medicare (always denied). Both errors happen at check-in or scheduling, not in billing.
Coordination of Benefits in Optometry: Billing Medical and Vision
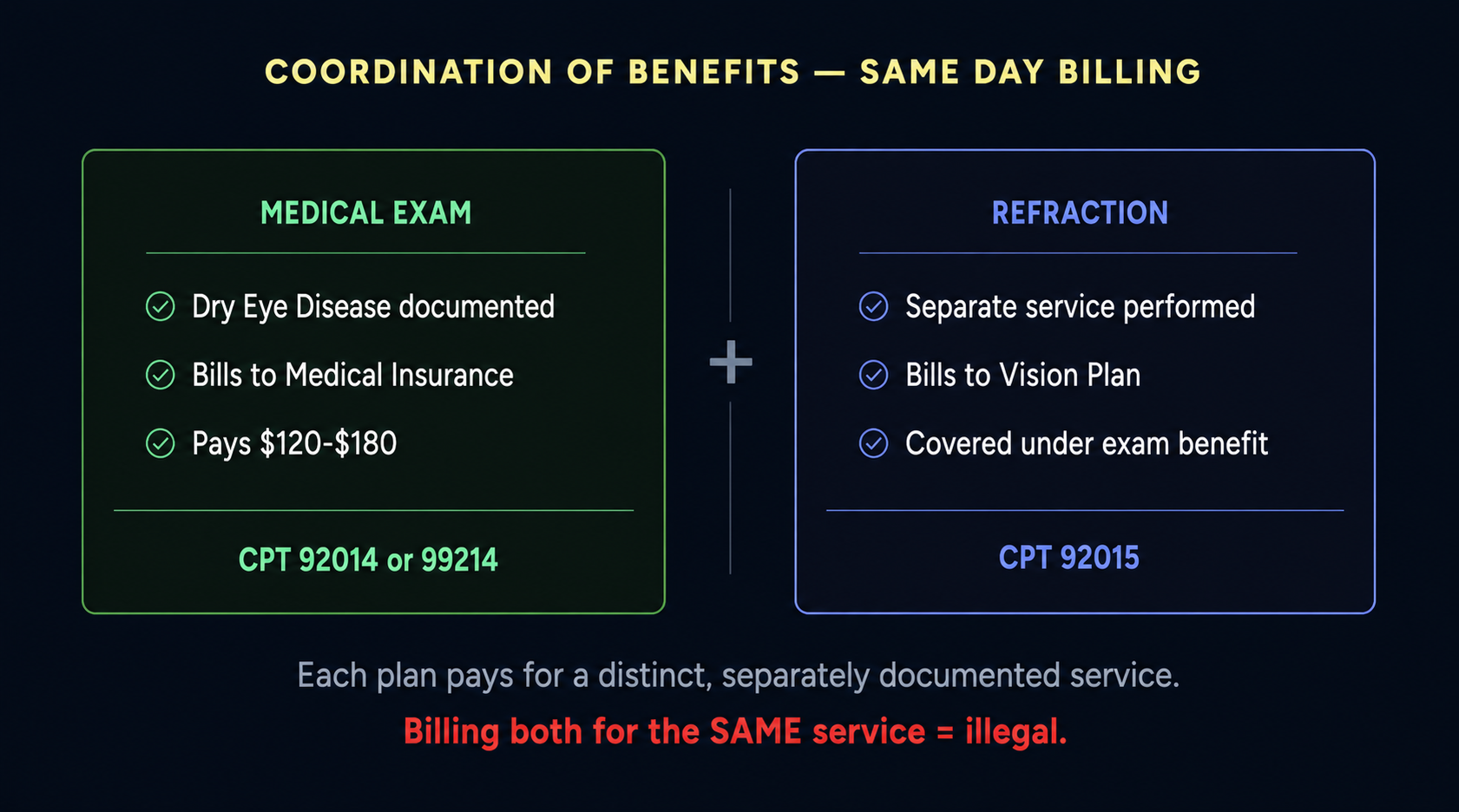
COB is the process of billing both a patient's vision plan and their medical insurance when distinct services were performed for each in the same visit. It is legal, appropriate, and systematically underdone in independent optometry practices.
A patient presents with dry eye disease and also requests a refraction. The medical examination goes to medical insurance. The refraction goes to the vision plan as a separate claim. Two distinct services, each with its own documentation, each billed to the correct payer.
COMPLIANCE: Billing both plans for the same single service is illegal under federal law with civil monetary penalties up to $27,894 per false claim. COB is only legitimate when each payer receives a claim for a separately documented, distinct service. Source: AOA Coordination of Benefits guidance | CMS OPHTH-003
The COB fix starts at check-in, not in billing. If the front desk enters one plan and never flags dual coverage, billing never sees the COB opportunity.
KEY TAKEAWAY: Most practices bill one plan and leave the other uncollected on dual-coverage patients. The fix is flagging dual coverage at check-in, not in billing. Source: CMS Medicare Coverage of Optometry Services OPHTH-003
Medicare and Vision Billing: What Optometrists Need to Know
Medicare has specific rules for eye care that differ materially from commercial vision plans.
What Medicare does not cover: Routine eye exams. Refraction (CPT 92015) excluded by federal statute with no exceptions. Eyeglasses except in specific post-surgical situations.
What Medicare does cover: Annual dilated eye exams for diabetic patients once per year with documented diagnosis. Glaucoma screening for high-risk patients. Treatment of diagnosed eye disease. Medically necessary diagnostic testing.
The most common Medicare routing error: a diabetic Medicare patient presents and the front desk opens a vision supplement portal rather than Medicare. The visit qualifies as a medically necessary diabetic dilated eye exam under Medicare. The vision plan pays its contracted rate. Medicare would have paid significantly more. No denial arrives.
ABN REQUIREMENT: For any Medicare patient requesting a service Medicare does not cover, an Advance Beneficiary Notice must be signed before the service is delivered. Collecting without a signed ABN is a compliance violation regardless of the amount. Source: CMS OPHTH-003 | Medicare Benefit Policy Manual Chapter 15
KEY TAKEAWAY: If a Medicare patient presents with a medical complaint, route to Medicare first — not their vision supplement. The vision supplement covers routine services only. Getting this wrong silently costs the practice the difference between vision plan rates and Medicare rates on every qualifying encounter. Source: CMS Medicare Coverage of Optometry Services OPHTH-003
Top Vision Billing Mistakes That Cost Optometry Practices Revenue
**Mistake 1: Routing a Medical Encounter to the Vision Plan**
The most expensive and most invisible error in vision billing. A patient with a diagnosable medical condition gets routed to VSP at check-in. The vision plan processes the claim correctly at vision rates. No denial arrives. The practice collects a fraction of what the visit qualified for on medical insurance.
Practices where 85 percent or more of encounters are billed to vision plans regardless of the patient population have a systematic routing problem. That ratio alone represents significant annual collections forfeited per location. Source: Medical Billers and Coders, April 2026.
**Mistake 2: Billing CPT 92015 to Medicare**
Refraction is excluded from Medicare coverage by federal statute. This denial is automatic every time. Collecting from the patient without a signed ABN is a compliance violation regardless of the amount.
**Mistake 3: Billing 92014 for a Patient Who Qualifies as New**
A patient not seen in 36 or more months is a new patient. Billing 92014 instead of 92004 results in reduced reimbursement or denial. This compounds in any practice with patient retention gaps because nobody is checking the 36-month rule at check-in.
**Mistake 4: Missing Modifier 25 on Same-Day E/M and Procedure**
When a comprehensive eye exam and a procedure are performed in the same visit, Modifier 25 must be on the E/M code. Without it the payer bundles both services and pays for one. The missed revenue never triggers a denial.
**Mistake 5: Missing the COB Opportunity on Dual-Coverage Patients**
When a patient has both vision and medical insurance and distinct services are performed, both plans can be billed correctly. Most practices bill one and leave the other uncollected because dual coverage is never flagged at check-in.
KEY TAKEAWAY: All five mistakes share one root cause: a decision made at check-in before billing starts. Three of the five produce no denial at all. The revenue just closes at the wrong rate or never gets captured.
**How to Fix Vision Billing Errors at the Source**
Every error above traces back to one moment: the routing decision made at check-in before billing ever sees the visit.
Which insurance does this patient's visit belong to today? Medical or vision? Both? That decision gets made in 30 seconds by whoever is at the front desk without a written protocol, without a chief complaint check, and without any flag for dual coverage.
The fix is building a system around that decision rather than depending on a specific person. A written protocol at every intake station. A chief complaint question asked before insurance is selected. A dual-coverage flag in the check-in workflow. These changes do not require new software or additional staff. They require process.
A practice that corrected its intake-level billing workflow without hiring additional billing staff saw a 16 percent improvement in Net Collection Ratio within 90 days. The revenue was already there. It was being lost before billing ever saw the encounter. Source: Medical Billers and Coders, April 2026.
For the complete routing protocol including the decision tree and 5-question intake script, see the complete optometry billing guide.
**Frequently Asked Questions**
What is vision billing in optometry?
Vision billing is submitting claims to vision benefit plans including VSP, EyeMed, Davis Vision, Superior Vision, and Humana Vision for routine eye care services such as annual exams, refraction, contact lens fittings, and eyewear. It operates separately from medical billing and covers only wellness encounters with no diagnosed medical condition. The moment a visit involves a diagnosable eye condition, the encounter belongs on medical insurance, not a vision plan.
What is the difference between vision billing and medical billing?
Vision billing covers routine wellness encounters reimbursed at contracted rates by vision plans, typically a fraction of what medical insurance pays, with a frequency limit of once every 12 to 24 months. Medical billing covers encounters driven by a diagnosed eye condition reimbursed at significantly higher rates by medical insurance with no frequency cap. The chief complaint determines which applies, not which insurance card the patient presents at check-in.
What CPT codes are used in vision billing?
The primary exam codes are 92002 and 92004 for new patients and 92012 and 92014 for established patients. Refraction uses CPT 92015. Contact lens fitting codes run from 92310 to 92317 depending on lens type. Optical dispensing uses V-codes starting at V2020. CPT 92015 is never covered by Medicare regardless of the patient's other vision coverage. A patient not seen in 36 or more months qualifies as new and should be billed under 92004 not 92014.
Can you bill vision and medical insurance on the same day?
Yes, when distinct services are separately performed and documented. A medical exam for dry eye disease can go to medical insurance while a refraction performed in the same visit goes to the vision plan. Billing both plans for the exact same single service is illegal under federal law with civil monetary penalties up to $27,894 per false claim. Each claim must reflect a separately documented, distinct service with its own CPT code and clinical basis.
Why do vision billing claims get denied?
The most common causes are billing a medical ICD-10 code on a vision plan claim, wrong CPT code for patient type, billing CPT 92015 to Medicare, submitting after the frequency limit is exhausted, and filing both plans for the same service without separate documentation. The most expensive errors are not denials but silent underpayments from routing medical encounters to vision plans, which pay at the wrong rate with no flag.
Does Medicare cover vision billing?
Medicare does not cover routine eye exams, refraction, or eyeglasses. It covers medically necessary eye care including annual dilated eye exams for diabetic patients, glaucoma screening for high-risk patients, and treatment of diagnosed eye conditions at medically necessary frequency. Billing CPT 92015 to Medicare always denies. Medicare patients requesting routine services not covered by Medicare must sign an Advance Beneficiary Notice before the service is delivered.